
The Algorithm is Denying Your Auth Request
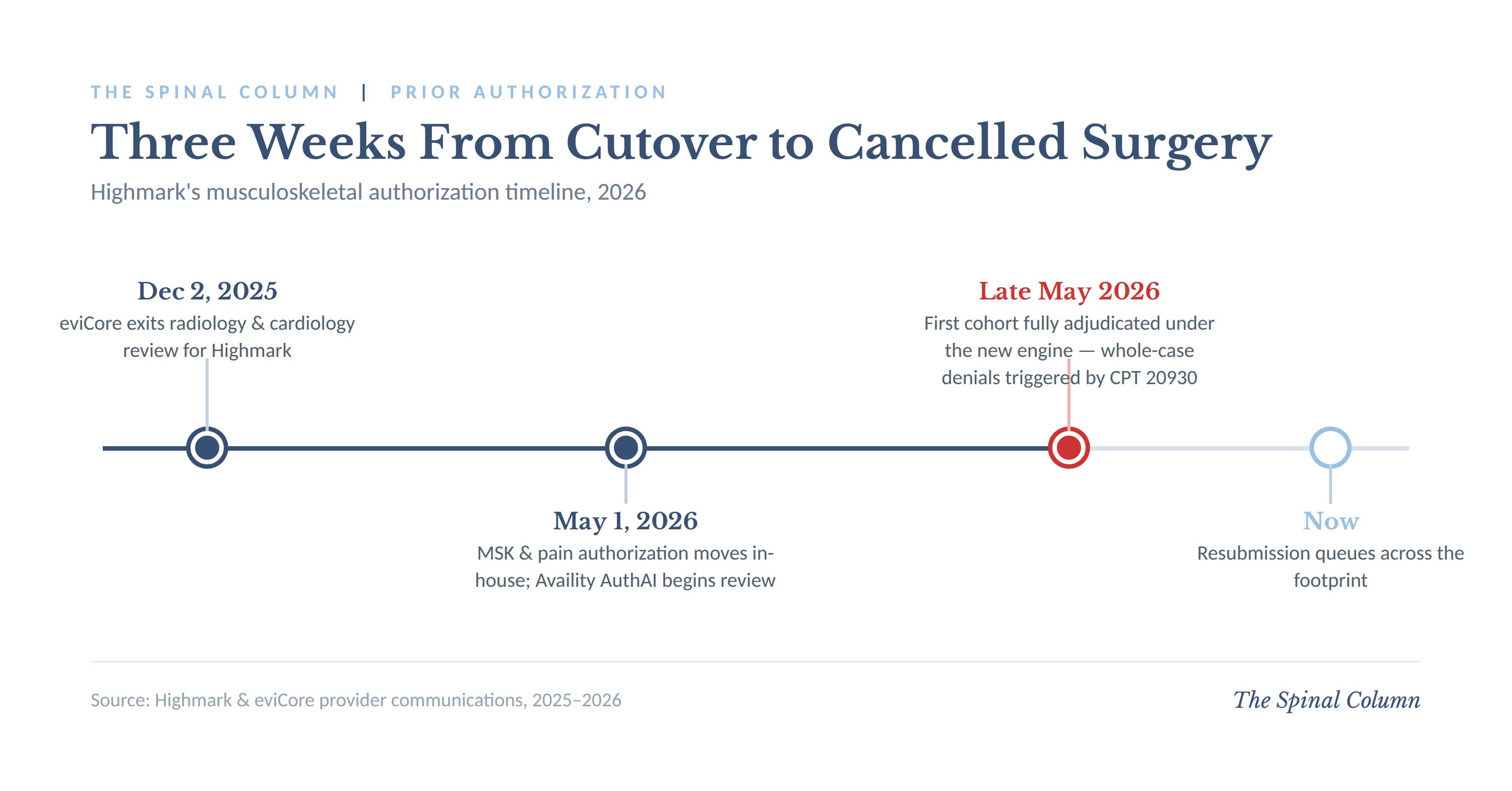
Highmark moved musculoskeletal prior authorization in-house on May 1. Three weeks later, an add-on code that Medicare hasn’t paid separately in decades started cancelling my spine surgeries.

This month, my office began seeing something I had not seen in a seven years of practice. Fusion authorizations were coming back denied — not pended, not questioned, denied — and kicked back for resubmission. The trigger appeared to be CPT 20930, the morselized allograft add-on code. I have watched payers bundle 20930, ignore it, zero it out, and pay it at trivial rates. I had never watched it stand between a patient and the operating room. A bundled add-on code with no relative value units under the Medicare fee schedule was now functioning as a stop sign on the whole case.
If you practice in the Highmark footprint, you are probably seeing it too. The timing is not a coincidence, and the mechanism is worth understanding, because it tells you something about where prior authorization is heading for all of us. It is also instructive for young spine surgeons to understand this code, so I will dig into this as well.
What changed on May 1
Effective May 1, 2026, eviCore no longer processes musculoskeletal, joint, and spine surgery prior authorization requests on behalf of Highmark.¹ Highmark moved the function in-house. Providers now submit musculoskeletal and interventional pain management authorization requests through Availity Essentials, and Highmark is using Availity’s AuthAI tool to review them.² The submission path runs from Availity Essentials into Predictal and then onto the Helion Arc technology platform for processing.³ Highmark’s own provider communications describe the goal as faster, more streamlined determinations with redundancies eliminated.²
The denials in my office clustered roughly three weeks after the cutover — the first cohort of cases adjudicated start-to-finish under the new engine. That sequence matters. This is not a coverage policy that changed. The policies governing 20930 did not move. What changed is the thing reading the request.
The cost nobody bills
To understand why this code in particular became a tripwire, you have to follow the money, and the money is not where most surgeons think it is.
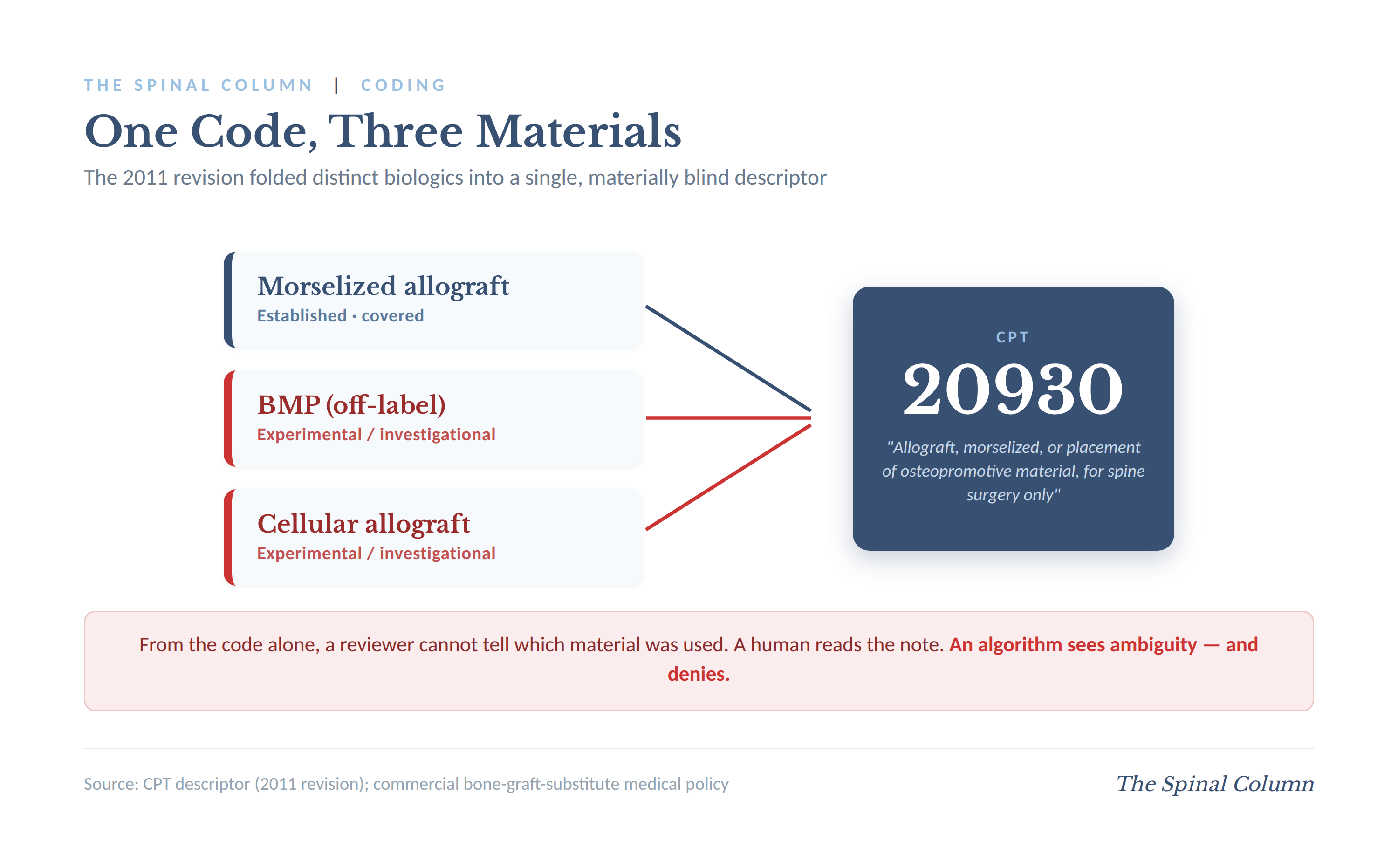
The biologic you place has no code of its own. There is no CPT or HCPCS code for bone morphogenetic protein; when CPT 20930 was revised in 2011 to include BMP-type materials used in spine surgery, the material folded into the add-on code rather than getting its own line.⁴ Demineralized bone matrix, cellular allograft, osteopromotive putty — they all collapse into the same descriptor. There is no separate line item that reimburses the substance itself.
On the facility side, the material is absorbed. For inpatient cases, Medicare pays the hospital through one MS-DRG for the entire stay; the facility may report an ICD-10-PCS code for BMP placement if it wants, but the payment group does not flex because you opened a kit.⁵ The DRG does not widen for a $5,000 BMP. The comprehensive APC does not widen in the hospital outpatient department. The ASC rate does not widen, and the ASC rate is the thinnest of the three. The hospital buys the material and the hospital eats it.
This produced a quiet equilibrium that held for two decades. Payers wrote experimental/investigational policies they rarely enforced at the facility level, because there was nothing to enforce against — the biologic was invisible inside the bundle. Facilities treated biologics as a known overhead line. Surgeons chose grafts on clinical judgment. The system functioned, in large part, because nobody was actually billing the thing the policies were written to restrict.
The permission slip, not the invoice
Here is where a reasonable assumption goes wrong, and I want to correct it because I made the same one.
When a payer approves your 20930 and tells you that you may use demineralized bone matrix but not BMP or cellular allograft, it looks like they are paying for one material and not the other. They are not paying for either. The material-specific approval is a medical-necessity gate, not a payment decision. It is a permission slip telling you what you are allowed to implant without triggering a denial — not an invoice reimbursing what you implanted.
Approval means the claim survives. Denial means the payer considers that use of 20930 experimental/investigational, and depending on the payer, that designation can contaminate the linked fusion claim on audit. Highmark’s commercial policy S-235 lists a long roster of bone graft substitutes as experimental/investigational and non-covered, and states plainly that procedure code 20930 is not a stand-alone procedure and must be used with a primary spinal procedure code.⁶ The cost of the graft is sunk into the facility bundle regardless of which way the gate swings. Demineralized bone matrix included.
The professional fee is a separate, smaller stream, and it is the only place a check actually changes hands. Unlike Medicare, where 20930 carries a status “B” designation, no RVUs, and is never separately paid,⁷ the National Correct Coding Initiative does not bundle 20930 into the arthrodesis codes, and commercial payers may reimburse a modest professional allowable for it.⁸ That allowable pays you for the minutes of work placing graft. It does not pay for the substance, and it is not what the medical-necessity gate is adjudicating.
The code that can’t tell the algorithm what it is
Now the mechanism is clear.
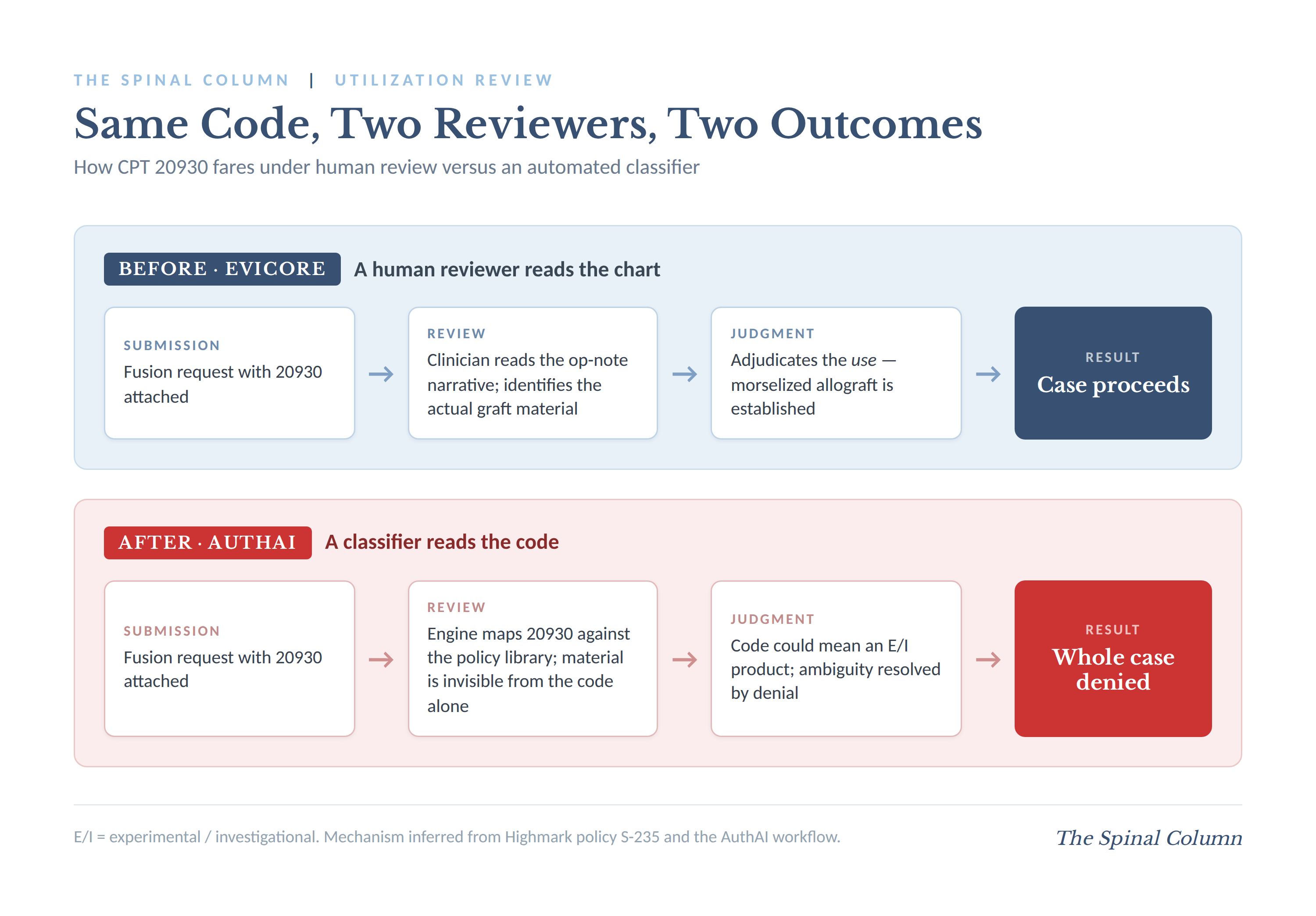
The 2011 revision that folded morselized allograft, osteopromotive material, BMP, and cellular products into a single descriptor created a code that is materially blind. From the code alone, you cannot tell whether 20930 represents a covered cadaver allograft or an experimental cellular product. The payer can only learn the material from the operative note or the authorization narrative.
A human reviewer at eviCore read that narrative and adjudicated the use. AuthAI sees a code that could be any of three materials — at least two of which sit in an experimental/investigational policy — and resolves the ambiguity the only way an unsupervised classifier can resolve it, by denying. The structural flaw is not unique to Highmark. It is latent in every payer’s policy library, because every payer inherited the same materially blind code in 2011. Automated review is simply the thing that activates the flaw. This fits a pattern that spine surgeons are going to see repeatedly as payers replace human utilization reviewers with natural-language classifiers: the codes most vulnerable to algorithmic denial are the ambiguous ones, and our specialty is full of them.
The denial is not a coverage judgment. It is the result of an algorithmic classification error driven by the new platform.
What to do about it
Audit your submissions. Check whether 20930 is even on your Highmark authorization requests. As an add-on with negligible professional allowable and no separate authorization requirement on Highmark’s procedure list, it may not need to be there at all. You can still report it on the claim.
Scrub the narrative. When the material is morselized allograft, document morselized allograft plainly. Marketing language for osteobiologic products in an auth packet is exactly the signal a classifier is built to flag.
Demand peer-to-peer on every whole-case denial. Highmark provides the opportunity to discuss a utilization review denial with a licensed, board-certified clinical peer reviewer, connected directly to the reviewer involved in the determination.⁹ Make a physician put a name on an algorithm’s denial of a medically necessary fusion.
Document the pattern. Record dates, codes submitted, denial language, and resubmission outcomes. Pennsylvania’s Act 146 of 2022 requires that a prior authorization denial — other than an administrative denial — be issued by a licensed reviewer with training in the same or similar specialty that typically manages the service in question, or one consulting with such a reviewer, and it extends the same standard to peer-to-peer review.¹⁰ Whether an automated determination satisfies that standard is a question the Pennsylvania Insurance Department has jurisdiction to investigate.¹⁰
Report it. A simultaneous cutover means the entire footprint hit this wall at once. Your state medical society and your specialty societies should hear about clusters, with specifics.
Where this leaves us
A payer moving authorization in-house and layering an AI engine on top of it is not, by itself, a problem. Done competently, it could be faster for everyone. Competent deployment would validate the new engine against eviCore’s historical approval patterns before going live, route discordant determinations to human review rather than auto-denying them, and build a rule that a zero-RVU add-on code can never cancel the primary arthrodesis it is attached to. None of that is exotic. It is the ordinary diligence you would expect before handing surgical authorization to a classifier.
If resubmission queues are filling across Pennsylvania three weeks into the new system, over a code that has been bundled and ignored since the Clinton administration, it would suggest that the validation step is essentially the part that got skipped.
Edward M. DelSole, MD, FAAOS, is a fellowship-trained orthopaedic spine surgeon at Keystone Spine and Pain Management in Reading, Pennsylvania.
References
EviCore by Evernorth. Highmark Provider Resources. “Effective May 1, 2026, EviCore will no longer process Musculoskeletal Pain Management, Joint and Spine Surgery prior authorization requests on behalf of Highmark.” evicore.com/resources/healthplan/highmark
Highmark Provider News. “MSK Authorization Will Transition from eviCore to Highmark on May 1, 2026.” February 2026. providers.highmark.com/communications-hub/news-and-updates/msk-authorization-will-transition-from-evicore-to-highmark
Highmark. “Provider Portal FAQs: Authorization Process via Availity Essentials.” February 2026. providers.highmark.com/content/dam/highmark/en/providerresourcecenter/pdfs/all/documents/pdfs/claims-and-authorization/authorization-guidance/authorization-process-faqs.pdf
Blue Cross Blue Shield of North Carolina. Corporate Medical Policy: Bone Morphogenetic Protein. “In 2011, CPT code 20930 was revised to include BMP-type materials used in spine surgery.” bluecrossnc.com/providers/policies-guidelines-codes/commercial/surgery/updates/bone-morphogenetic-protein
Medtronic. Infuse Bone Graft Billing and Coding Guide. Citing AHA Coding Clinic for ICD-10-CM and ICD-10-PCS, First Quarter 2018; MS-DRG payment methodology. medtronic.com (reimbursement resources)
Highmark Commercial Medical Policy S-235: Bone Graft Substitutes. “Procedure Code 20930 is not a stand-alone procedure and must be used separately with a primary spinal procedure code.” securecms.highmark.com/content/medpolicy/en/highmark/pa/commercial/policies/Surgery/S-235
Select Health Medical Coding Policy CR-57: Autograft & Allograft for Spine Surgery. “Medicare considers codes 20930 and 20936 ‘B’ Status codes and has not assigned any RVUs.” Also KZA Coding Coaches, “Denials of 20930 and 20936,” March 2026.
AAPC Orthopedic Coding Alert. “Separately Report Grafting During Arthrodesis”; “Reader Questions: Don’t Charge Medicare for These Bone Grafts.” NCCI does not bundle 20930 into 22612/22630; private payers may reimburse 20930.
Highmark Provider News. “Important Highmark Reminders: Utilization Review, Patient Notification, and More.” March 2026. Clinical peer reviewers are licensed, board-certified physicians available to discuss denial determinations. providers.highmark.com/communications-hub/news-and-updates/highmark-reminders-utilization-review-patient-notification-and-more
Act of November 3, 2022 (Act 146), amending the Insurance Company Law of 1921; Section 2155(d)–(e), 40 P.S. § 991.2155(d)–(e). Insurer denial reviewers and peer-to-peer reviewers must be licensed health care providers “with appropriate training, knowledge or experience in the same or similar specialty that typically manages or consults on the health care service in question.” Enforcement authority at 40 P.S. §§ 991.2181(d), 991.2182. See Pennsylvania Insurance Department implementation notice, Pennsylvania Bulletin, Vol. 54, No. 30 (July 27, 2024); Pennsylvania Medical Society (PAMED), “Insurance Department Act 146 Implementation of Prior Authorization Provisions,” Notice 2024-11.